Reimagining Stroke Recovery Through Performance Metrics
The Next Frontier for the Neurologic Longevity Athlete

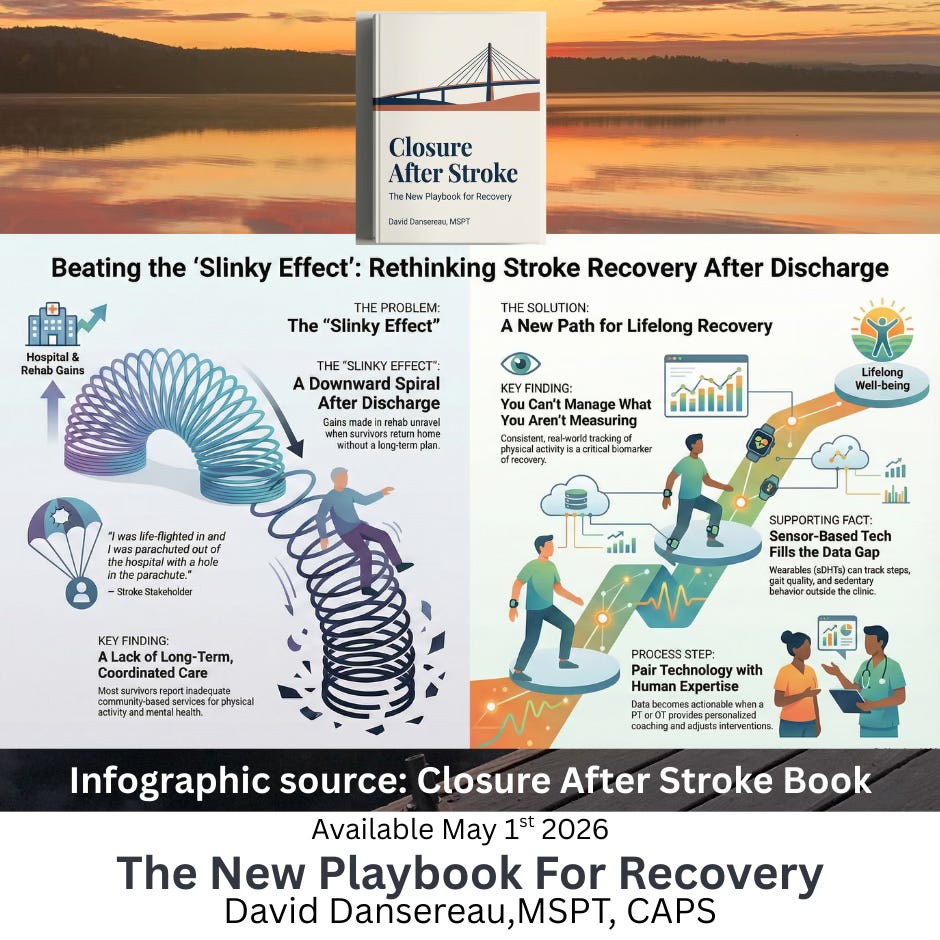
After a stroke, the medical system often treats recovery as a race with a fixed finish line—typically coinciding with insurance expiration or hospital discharge to make room for the next patient. This episodic model leaves survivors at risk of the “Slinky Effect,” a downward spiral where physical gains building during therapy unravel once structured support is withdrawn. To achieve true “Closure After Stroke,” we must pivot from a reactive rehabilitation mindset to a proactive, athletic performance model.

The Paradigm Shift: From Stroke Patient to Longevity Athlete
In the world of professional sports, athletes undergo annual “combines” or screenings as they return to training camp each year to detect subtle imbalances before they jump on the field unprepared and become career-ending injuries.
In fact, in my early PT days working with athletes and partnering with sports performance and remote assessment technologies, we offered mobility screens to professional elite soccer players here in the US with Major League Soccer (MLS) and in the UK in the British Premiere League. This athlete monitoring was offered during the off-season as well to monitor subtle performance signals and flag declines in joint range of motion (ROM) and agility before any injuries even developed. I dive into this technology and how we could harness these same technologies for stroke in my new book.
We must apply this same rigor to stroke survivors, viewing them not as “recovered patients,” “safe for discharge to home” but as longevity athletes managing a chronic condition.-David Dansereau, MSPT, CAPS Author Closure After Stroke
The Dental Model of Stroke Care
A guest of our podcast, Dr. Teresa Jacobson Kimberley brilliantly advocates for a “Dental Model,” where survivors receive intense rehabilitation annually (e.g., six weeks) and routine check-ups twice a year for life. This ensures survivors are managed for their entire lifespan, rather than being “dropped off a cliff” after the acute phase. If you missed our conversation with her on our podcast, tune in here or link below to the deep dive from leading PT experts we’ve interviewed.
Movement as Essential Medicine
Just as diabetes is managed with insulin and A1C tracking, mobility and physical activity must be treated as "essential medicine" for stroke survivors. This requires treating physical therapists (PTs) as "movement scientists" who teach survivors how to monitor and maintain their health-span for life.
The Framework for Annual Mobility Assessments
An annual stroke mobility assessment should move beyond basic gait speed to a high-resolution “performance screen” using Sensor-Based Digital Health Technologies (sDHTs).
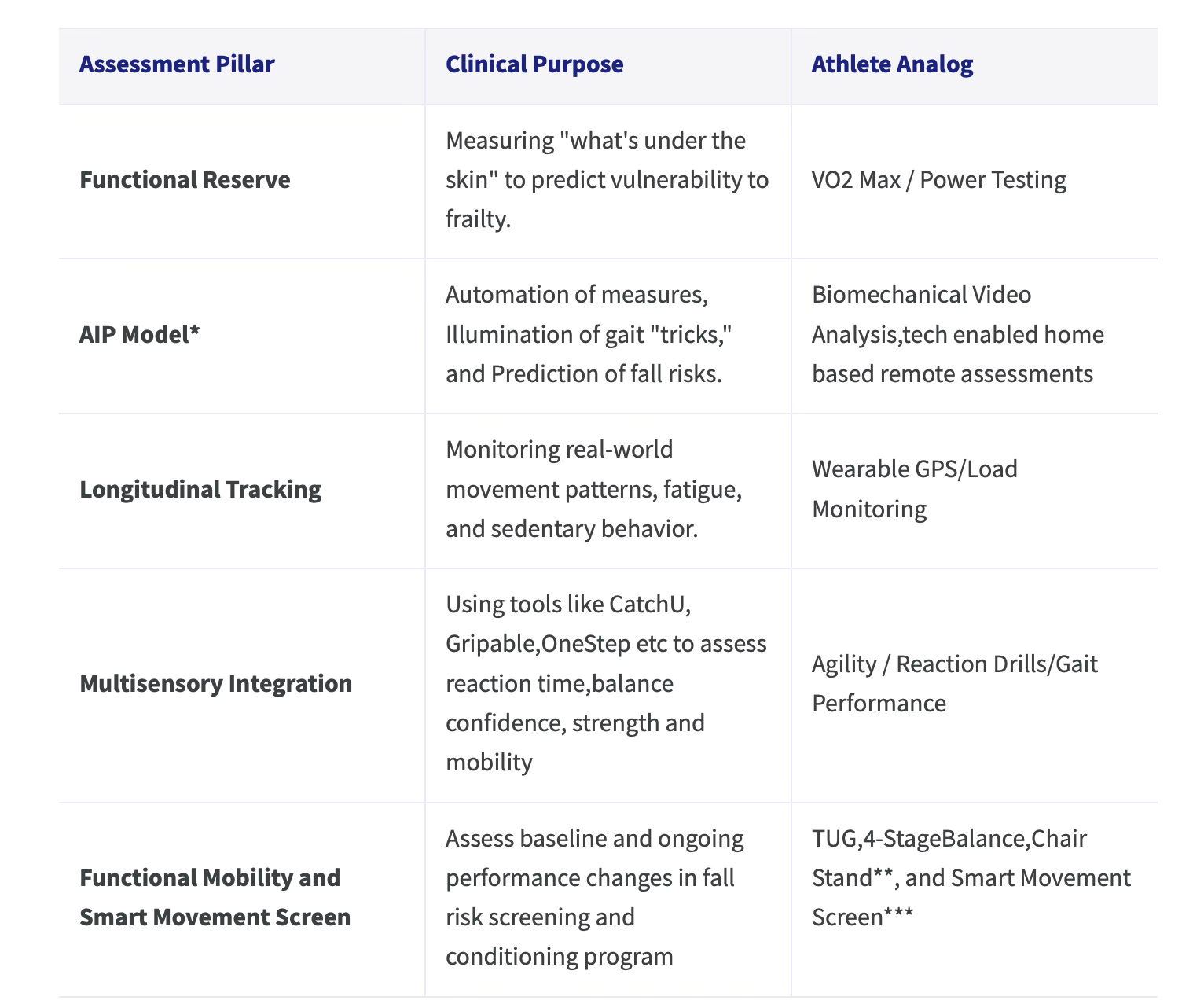
* The AIP Model is a framework developed by Dr. Arun Jayaraman of the Shirley Ryan AbilityLab for how Sensor-Based Digital Health Technologies (sDHTs) function to measure and manage stroke recovery in both hospital and home settings.
** Believe in Balance Course Module-Fall Screening and Conditioning Program by David Dansereau,MSPT,CAPS
*** Body in Balance Book and Achieve Balance Course by David Dansereau,MSPT,CAPS
The Role of sDHT: The "Glucose Monitor" for Movement
The primary obstacle to this model has been the “subjective snapshot” of the clinic visit. sDHTs replace this with an objective, continuous “movie” of a survivor’s health.
Automation: Sensors can predict scores for the six-minute walk test or other evidence based fall risk screen in just one minute of activity.
Illumination: They distinguish between genuine motor recovery and “trick movements” that might cause long-term orthopedic damage.
Prediction: Machine learning can use Day 1 sensor data to predict fall risk a year post-stroke.
Correction: Devices like the MyHand system use sensors to provide real-time feedback, ensuring neuroplasticity is driven by correct movement patterns.
Case Study: Data-Driven Recovery with Rory Polera
Rory Polera serves as a prime example of a “longevity athlete.” By “hacking” his recovery with a suite of wearables—including Oura, Apple Watch, Continuous Glucose Monitors (CGMs),SPO2 sensors and Ai insights—he transitioned from a passive recipient of care to an active manager of his recovery data. His experience highlights that the choice to engage with technology can empower a survivor to conduct an “ethnography of oneself,” turning recovery into a learning lab.
Conclusion: A Call for Surveillance in Stroke Care
True closure in stroke recovery requires a system of longitudinal surveillance similar to cancer or diabetes care. By implementing annual mobility assessments, we catch declines early, adjust the “dosage” of physical activity (our best medicine!) and empower survivors to maintain their independence for the rest of their lives.
For a deeper dive on this topic read more:
Author Note: This chapter will be further developed and referenced in my upcoming book, Closure after Stroke and presented in an upcoming LiveStream for subscribers on Achieve Balance by SmartMovesPT within my Believe in Balance Course.